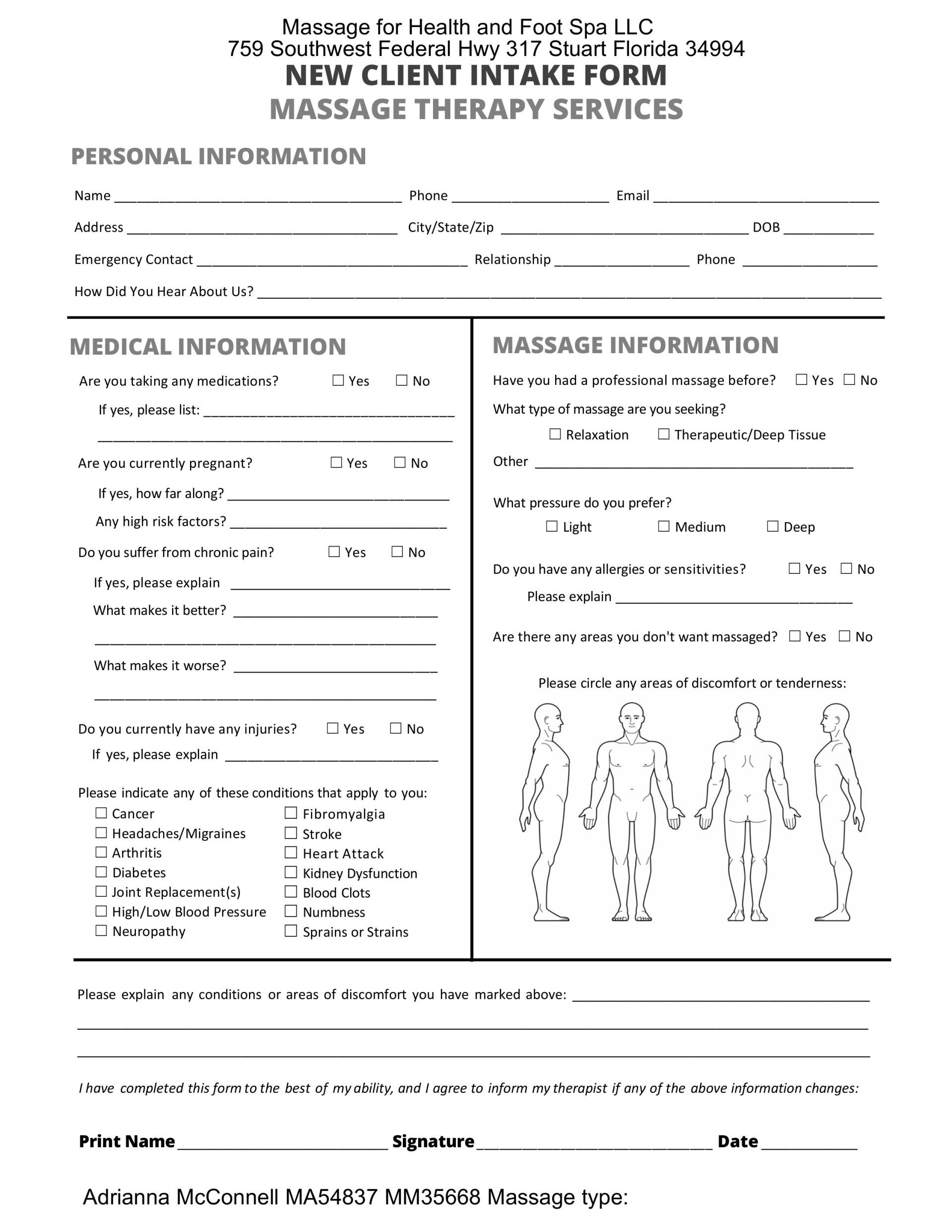
Massage for Health and Foot Spa LLC
759 Southwest Federal Highway #317 Stuart Florida 34994
Adrianna McConnell MA54837 MM35668
Location
759 SW Federal Hwy 317
34994 Stuart
Adrianna McConnell MA54837 MM35668
759 SW Federal Hwy 317
34994 Stuart